

")


双能量计算机断层扫描的原理和在膀胱癌中的新应用
- 作者: Masino F.1, Eusebi L.2, Montatore M.1, Muscatella G.1, Gifuni R.1, Ferrara V.2, Marcellini M.3, Guglielmi G.1,4,5
-
隶属关系:
- Foggia University School of Medicine
- “Carlo Urbani” Hospital
- “Senigallia” Hospital
- “Dimiccoli” Hospital
- “IRCCS Casa Sollievo della Sofferenza” Hospital
- 期: 卷 5, 编号 3 (2024)
- 页面: 551-566
- 栏目: 科学评论
- URL: https://bakhtiniada.ru/DD/article/view/310037
- DOI: https://doi.org/10.17816/DD625405
- ID: 310037
如何引用文章
全文:

详细
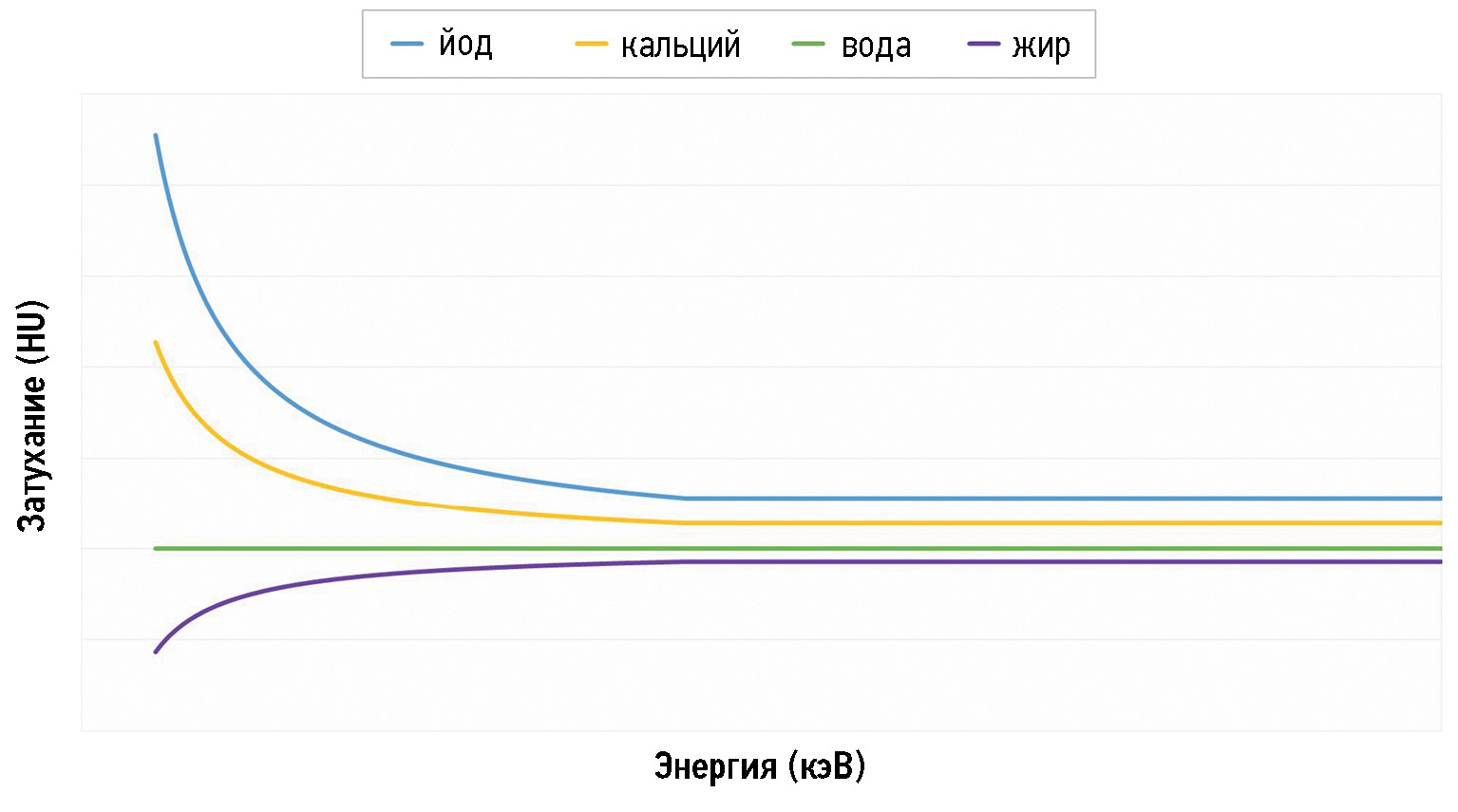
目前,膀胱癌患者最常见的仪器检查方法是使用计算机断层扫描和多参数磁共振成像进行尿路造影。但是,最近双能量计算机断层扫描已越来越多地用于诊断癌症。这篇概述性的文章简要描述双能量计算机断层扫描的各个方面,如物理操作原理、工作方法、规程和图像处理方法,为了这一先进技术应用于前景广阔的膀胱癌诊断领域,形成总体的认识。特别是,研究使用双能计算机断层扫描来比较基本图像(如碘图)与使用标准计算机断层扫描获得的图像的可行性。
双能量计算机断层扫描可用于膀胱癌的诊断、分期和治疗规划。然而,由于医疗机构中相应设备不足,以及缺乏受过训练的人员来正确进行检查,并恰当的描述检查结果,该方法的使用受到了限制。
关键词
作者简介
Federica Masino
Foggia University School of Medicine
Email: federicamasino@gmail.com
ORCID iD: 0009-0004-4289-3289
MD
意大利, FoggiaLaura Eusebi
“Carlo Urbani” Hospital
Email: lauraeu@virgilio.it
ORCID iD: 0000-0002-4172-5126
MD
意大利, JesiManuela Montatore
Foggia University School of Medicine
Email: manuela.montatore@unifg.it
ORCID iD: 0009-0002-1526-5047
MD
意大利, FoggiaGianmichele Muscatella
Foggia University School of Medicine
Email: muscatella94@gmail.com
ORCID iD: 0009-0004-3535-5802
MD
意大利, FoggiaRossella Gifuni
Foggia University School of Medicine
Email: rossella.gifuni@unifg.it
ORCID iD: 0009-0009-9679-3861
MD
意大利, FoggiaVincenzo Ferrara
“Carlo Urbani” Hospital
Email: vincenzoferrara4@gmail.com
ORCID iD: 0000-0001-8625-4308
MD
意大利, JesiMassimo Marcellini
“Senigallia” Hospital
Email: massimo.marcellini@sanita.marche.it
ORCID iD: 0000-0002-5281-7819
MD
意大利, SenigalliaGiuseppe Guglielmi
Foggia University School of Medicine; “Dimiccoli” Hospital; “IRCCS Casa Sollievo della Sofferenza” Hospital
编辑信件的主要联系方式.
Email: giuseppe.guglielmi@unifg.it
ORCID iD: 0000-0002-4325-8330
MD, Professor
意大利, Foggia; Barletta; San Giovanni Rotondo参考
- Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71(3):209–249. doi: 10.3322/caac.21660
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70(1):7–30. doi: 10.3322/caac.21590
- Soria F, Shariat SF, Lerner SP, et al. Epidemiology, diagnosis, preoperative evaluation and prognostic assessment of upper-tract urothelial carcinoma (UTUC). World J Urol. 2017;35(3):379–387. doi: 10.1007/s00345-016-1928-x
- Verma S, Rajesh A, Prasad SR, et al. Urinary bladder cancer: role of MR imaging. Radiographics. 2012;32(2):371–387. doi: 10.1148/rg.322115125
- Rouprêt M, Babjuk M, Burger M, et al. European Association of Urology Guidelines on Upper Urinary Tract Urothelial Carcinoma: 2020 Update. Eur Urol. 2021;79(1):62–79. doi: 10.1016/j.eururo.2020.05.042
- Farling KB. Bladder cancer: Risk factors, diagnosis, and management. Nurse Pract. 2017;42(3):26–33. doi: 10.1097/01.NPR.0000512251.61454.5c
- Eusebi L, Masino F, Gifuni R, et al. Role of multiparametric-MRI in bladder cancer. Current Radiology Reports. 2023;11(5):69–80. doi: 10.1007/s40134-023-00412-5
- Babjuk M, Burger M, Capoun O, et al. European Association of Urology Guidelines on Non-muscle-invasive Bladder Cancer (Ta, T1, and Carcinoma in Situ). Eur Urol. 2022;81(1):75–94. doi: 10.1016/j.eururo.2021.08.010
- Babjuk M, Böhle A, Burger M, et al. EAU Guidelines on Non-Muscle-invasive Urothelial Carcinoma of the Bladder: Update 2016. Eur Urol. 2017;71(3):447–461. doi: 10.1016/j.eururo.2016.05.041
- Kamoun A, de Reyniès A, Allory Y, et al. A consensus molecular classification of muscle-invasive bladder cancer. European Urology. 2020;77(4):420–433. doi: 10.1016/j.eururo.2019.09.006
- Wang Z, Shang Y, Luan T, et al. Evaluation of the value of the VI-rads scoring system in assessing muscle infiltration by bladder cancer. Cancer Imaging. 2020;20(1). doi: 10.1186/s40644-020-00304-3
- Husband JE, Olliff JF, Williams MP, Heron CW, Cherryman GR. Bladder cancer: staging with CT and MR imaging. Radiology. 1989;173(2):435–440. doi: 10.1148/radiology.173.2.2798874
- Wong VK, Ganeshan D, Jensen CT, Devine CE. Imaging and management of Bladder Cancer. Cancers. 2021;13(6):1396. doi: 10.3390/cancers13061396
- Agrawal MD, Pinho DF, Kulkarni NM, et al. Oncologic applications of dual-energy CT in the abdomen. Radiographics. 2014;34(3):589–612. doi: 10.1148/rg.343135041
- Johnson T. Dual-Energy CT: General Principles. AJR Am J Roentgenol. 2012;199(5 Suppl):S3–S8. doi: 10.2214/AJR.12.9116
- Potenta SE, D’Agostino R, Sternberg KM, Tatsumi K, Perusse K. CT Urography for Evaluation of the Ureter. Radiogr Rev Publ Radiol Soc N Am Inc. 2015;35:709–726. doi: 10.1148/rg.2015140209
- Kawashima A, Vrtiska TJ, Leroy AJ, et al. CT Urography. Radiogr Rev Publ Radiol Soc N Am Inc. 2004;24:S35–S54. doi: 10.1148/rg.24si045513
- Caoili EM, Cohan RH. CT urography in evaluation of urothelial tumors of the kidney. Abdom. Radiol. 2016;41:1100–1107. doi: 10.1007/s00261-016-0695-x
- Cheng K, Cassidy F, Aganovic L, Taddonio M, Vahdat N. CT urography: How to optimize the technique. Abdom. Radiol. 2019;44:3786–3799. doi: 10.1007/s00261-019-02111-2
- Silverman SG, Leyendecker JR, Amis ES. What Is the Current Role of CT Urography and MR Urography in the Evaluation of the Urinary Tract? Radiology. 2009;250:309–323. doi: 10.1148/radiol.2502080534
- Shampain KL, Cohan RH, Caoili EM, Davenport MS, Ellis JH. Benign diseases of the urinary tract at CT and CT urography. Abdom. Radiol. 2019;44:3811–3826. doi: 10.1007/s00261-019-02108-x
- Metser U, Goldstein MA, Chawla TP, et al. Detection of urothelial tumors: Comparison of urothelial phase with excretory phase CT urography — a prospective study. Radiology. 2012;264(1):110–118. doi: 10.1148/radiol.12111623
- Kim JK, Park SY, Ahn HJ, Kim CS, Cho KS. Bladder cancer: analysis of multi-detector row helical CT enhancement pattern and accuracy in tumor detection and perivesical staging. Radiology. 2004;231(3):725–731. doi: 10.1148/radiol.2313021253
- Saksena MA, Dahl DM, Harisinghani MG. New imaging modalities in bladder cancer. World J Urol. 2006;24(5):473–480. doi: 10.1007/s00345-006-0118-7
- Parakh A, Lennartz S, An C, et al. Dual-Energy CT Images: Pearls and Pitfalls. Radiographics. 2021;41(1):98–119. doi: 10.1148/rg.2021200102
- Sauter A, Muenzel D, Dangelmaier J, et al. Dual-Layer Spectral Computed Tomography: Virtual Non-Contrast in Comparison to True Non-Contrast Images. Eur J Radiol. 2018;104:108–114. doi: 10.1016/j.ejrad.2018.05.007
- Ananthakrishnan L, Rajiah P, Ahn R, et al. Spectral Detector CT-Derived Virtual Non-Contrast Images: Comparison of Attenuation Values with Unenhanced CT. Abdom Radiol (NY). 2017;42(3):702–709. doi: 10.1007/s00261-016-1036-9
- Fornaro J, Leschka S, Hibbeln D, et al. Dual- and multi-energy CT: approach to functional imaging. Insights Imaging. 2011;2(2):149–159. doi: 10.1007/s13244-010-0057-0
- Silva AC, Morse BG, Hara AK, et al. Dual-energy (spectral) CT: applications in abdominal imaging. Radiographics. 2011;31(4):1031–1050. doi: 10.1148/rg.314105159
- Salameh JP, McInnes MDF, McGrath TA, Salameh G, Schieda N. Diagnostic Accuracy of Dual-Energy CT for Evaluation of Renal Masses: Systematic Review and Meta-Analysis. AJR Am J Roentgenol. 2019;212(4):W100–W105. doi: 10.2214/AJR.18.20527
- Ascenti G, Mazziotti S, Mileto A, et al. Dual-source dual-energy CT evaluation of complex cystic renal masses. AJR Am J Roentgenol. 2012;199(5):1026–1034. doi: 10.2214/AJR.11.7711
- Mileto A, Nelson RC, Samei E, et al. Impact of dual-energy multi-detector row CT with virtual monochromatic imaging on renal cyst pseudoenhancement: in vitro and in vivo study. Radiology. 2014;272(3):767–776. doi: 10.1148/radiol.14132856
- Chandarana H, Megibow AJ, Cohen BA, et al. Iodine quantification with dual-energy CT: phantom study and preliminary experience with renal masses. AJR Am J Roentgenol. 2011;196(6):W693–W700. doi: 10.2214/AJR.10.5541
- Tatsugami F, Higaki T, Nakamura Y, Honda Y, Awai K. Dual-energy CT: minimal essentials for radiologists. Jpn J Radiol. 2022;40(6):547–559. doi: 10.1007/s11604-021-01233-2
- Nolte-Ernsting C, Cowan N. Understanding multislice CT urography techniques: Many roads lead to Rome. Eur Radiol. 2006;16(12):2670–2686. doi: 10.1007/s00330-006-0386-z
- Ge X, Lan ZK, Chen J, Zhu SY. Effectiveness of contrast-enhanced ultrasound for detecting the staging and grading of bladder cancer: a systematic review and meta-analysis. Med Ultrason. 2021;23(1):29–35. doi: 10.11152/mu-2730
- Takahashi N, Vrtiska TJ, Kawashima A, et al. Detectability of urinary stones on virtual nonenhanced images generated at pyelographic-phase dual-energy CT. Radiology. 2010;256(1):184–190. doi: 10.1148/radiol.10091411
- Mangold S, Thomas C, Fenchel M, et al. Virtual nonenhanced dual-energy CT urography with tin-filter technology: determinants of detection of urinary calculi in the renal collecting system. Radiology. 2012;264(1):119–125. doi: 10.1148/radiol.12110851
- Coursey CA, Nelson RC, Boll DT, et al. Dual-energy multidetector CT: how does it work, what can it tell us, and when can we use it in abdominopelvic imaging? Radiographics. 2010;30(4):1037–1055. doi: 10.1148/rg.304095175
- Graser A, Johnson TR, Hecht EM, et al. Dual-energy CT in patients suspected of having renal masses: can virtual nonenhanced images replace true nonenhanced images? Radiology. 2009;252(2):433–440. doi: 10.1148/radiol.2522080557
- Nakagawa M, Naiki T, Naiki-Ito A, et al. Usefulness of advanced monoenergetic reconstruction technique in dual-energy computed tomography for detecting bladder cancer. Jpn J Radiol. 2022;40(2):177–183. doi: 10.1007/s11604-021-01195-5
- Patel BN, Vernuccio F, Meyer M, et al. Dual-Energy CT Material Density Iodine Quantification for Distinguishing Vascular From Nonvascular Renal Lesions: Normalization Reduces Intermanufacturer Threshold Variability. AJR Am J Roentgenol. 2019;212(2):366–376. doi: 10.2214/AJR.18.20115
- De Cecco CN, Darnell A, Rengo M, et al. Dual-energy CT: oncologic applications. AJR Am J Roentgenol. 2012;199(5S):S98–S105. doi: 10.2214/AJR.12.9207
- Vrtiska TJ, Takahashi N, Fletcher JG, et al. Genitourinary applications of dual-energy CT. AJR Am J Roentgenol. 2010;194(6):1434–1442. doi: 10.2214/AJR.10.4404
- Montatore M, Muscatella G, Eusebi L, et al. Current status on new technique and protocol in urinary stone disease. Current Radiology Reports. 2023;11:161–176. doi: 10.1007/s40134-023-00420-5
补充文件










