

")



Диагностические возможности компьютерной томографии сердца в предоперационной диагностике гипертрофической кардиомиопатии
- Авторы: Дарий О.Ю.1,2, Юрпольская Л.А.1, Рычина И.Е.1, Дорофеев А.В.1, Голухова Е.З.1
-
Учреждения:
- Национальный медицинский исследовательский центр сердечно-сосудистой хирургии имени А.Н. Бакулева
- Научно-практический клинический центр диагностики и телемедицинских технологий
- Выпуск: Том 5, № 3 (2024)
- Страницы: 467-479
- Раздел: Оригинальные исследования
- URL: https://bakhtiniada.ru/DD/article/view/310030
- DOI: https://doi.org/10.17816/DD629141
- ID: 310030
Цитировать
Полный текст

Аннотация
Обоснование. Комплексный подход изучения гипертрофической кардиомиопатии с помощью арсенала диагностической аппаратуры и новейших методик сканирования позволит обеспечить качественный контроль и эффективность лечения пациентов с гипертрофической кардиомиопатией. Актуальным и перспективным становится внедрение инновационных технологий и компьютерных вычислений на сканерах нового поколения для изучения фенотипических вариантов ремоделирования левого желудочка в сочетании с аномалиями хордо-папиллярного аппарата митрального клапана и структуры миокарда.
Цель — изучение возможностей компьютерной томографии в предоперационной диагностике фенотипических форм гипертрофической кардиомиопатии.
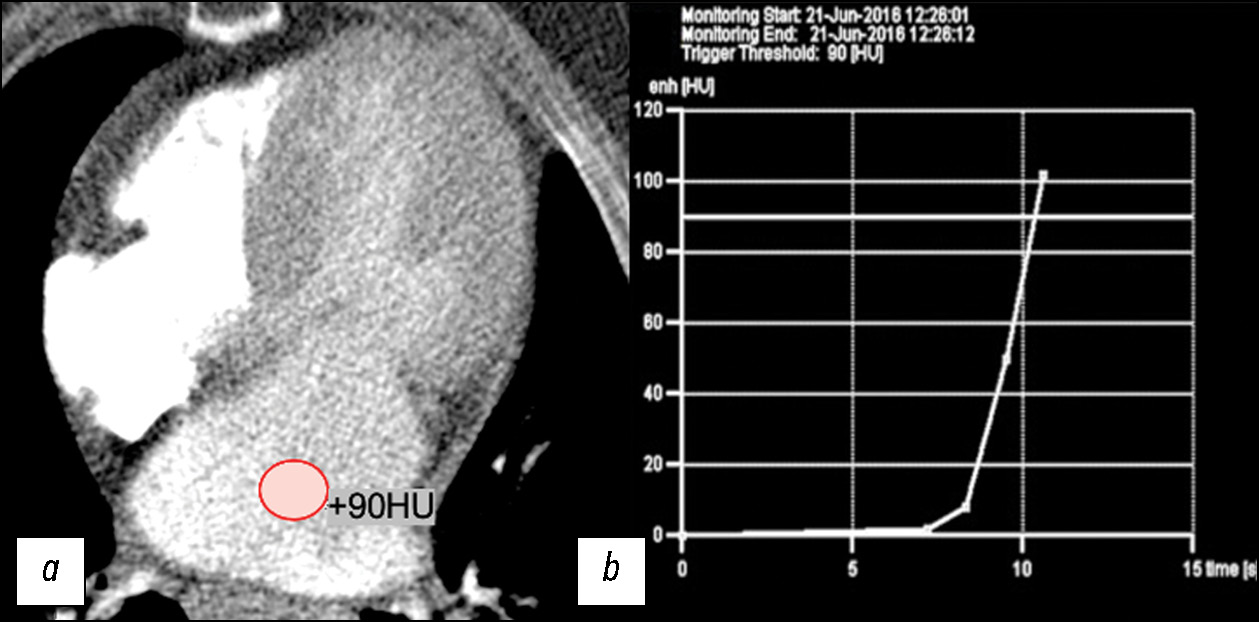
Материалы и методы. Проведён ретроспективный анализ данных 47 пациентов с гипертрофической кардиомиопатией (средний возраст 52±7 полных лет) перед хирургической коррекцией. Для изучения анатомии камер сердца и коронарных артерий, морфологии митрального клапана был применён разработанный нами протокол с автоматическим мониторингом болюса контрастного препарата в полости левого предсердия c пороговым значением 90 HU и двухфазным последовательным введением контрастного препарата. Для изучения структурных изменений миокарда проведен анализ данных полученных на двухэнергетическом компьютерном томографе с построением йодных карт отсроченного контрастирования. Всех пациентов с гипертрофической кардиомиопатией классифицировали на морфологические типы. В каждом случае оценивалась анатомия хордо-папиллярного аппарата.
Результаты. Наше исследование демонстрирует вариабельность фенотипических проявлений гипертрофической кардиомиопатии, условно разделённых на 5 морфологических типов и не ограниченных данными вариантами. 26 (55%) пациентов имели диффузно-септальный морфологический фенотип гипертрофической кардиомиопатии. Среднежелудочковый выявлен у 5 (11%) пациентов, из них среднежелудочковый фенотип с апикальным выпячиванием/аневризмой левого желудочка у 2 (4%). У 8 (18%) пациентов выявлен фокально-базальный фенотип, у 4 (8%) пациентов — концентрический фенотип, и еще у 4 (8%) — апикальный фенотип. У большинства обследованных диагностированы аномалии хордо-папиллярного аппарата митрального клапана, разделённые на аномалии количества и положения папиллярных мышц, а также соотношения хорд и мышц. Интрамиокардиальный ход коронарных артерий выявлен у 10 (21%) пациентов, из них у 3 (14%) отмечались признаки динамического сужения. У всех пациентов выявлены очаговые накопления йода на картах отсроченного контрастирования. У 10 из 13 (76%) пациентов значение фракции внеклеточного объёма ECV превышало нормальные диапазоны. Среднее значение ECV миокарда левого желудочка, по данным двухэнергетической компьютерной томографии, — 30,58% (95% доверительный интервал 27–34%).
Заключение. Разработанные нами протоколы сканирования на компьютерных томографах разных поколений позволяют определить характерные паттерны морфологических типов гипертрофической кардиомиопатии в одном исследовании и детально интерпретировать геометрию камер и клапанной системы сердца, функцию левого желудочка и состояние коронарного русла, а кроме того — структурные изменения миокарда левого желудочка.
Полный текст
Открыть статью на сайте журналаОб авторах
Ольга Юрьевна Дарий
Национальный медицинский исследовательский центр сердечно-сосудистой хирургии имени А.Н. Бакулева; Научно-практический клинический центр диагностики и телемедицинских технологий
Email: dariiolyka@mail.ru
ORCID iD: 0000-0003-0140-8166
SPIN-код: 1844-4944
канд. мед. наук
Россия, Москва; МоскваЛюдмила Анатольевна Юрпольская
Национальный медицинский исследовательский центр сердечно-сосудистой хирургии имени А.Н. Бакулева
Email: layurpolskaya@bakulev.ru
ORCID iD: 0000-0001-7780-2405
SPIN-код: 8436-9665
д-р мед. наук
Россия, МоскваИнна Евгеньевна Рычина
Национальный медицинский исследовательский центр сердечно-сосудистой хирургии имени А.Н. Бакулева
Email: ierychina@bakulev.ru
ORCID iD: 0000-0001-8056-4188
SPIN-код: 3516-0729
канд. мед. наук
Россия, МоскваАлексей Владимирович Дорофеев
Национальный медицинский исследовательский центр сердечно-сосудистой хирургии имени А.Н. Бакулева
Email: avdorofeev@bakulev.ru
ORCID iD: 0000-0003-0833-9650
канд. мед. наук
Россия, МоскваЕлена Зеликовна Голухова
Национальный медицинский исследовательский центр сердечно-сосудистой хирургии имени А.Н. Бакулева
Автор, ответственный за переписку.
Email: egolukhova@bakulev.ru
ORCID iD: 0000-0002-6252-0322
SPIN-код: 9334-5672
д-р мед. наук, профессор, академик РАН
Россия, МоскваСписок литературы
- Maron B.J., McKenna W.J., Danielson G.K., et al. American College of Cardiology/European Society of Cardiology Clinical Expert Consensus Document on Hypertrophic Cardiomyopathy // J Am Coll Cardiol. 2003. Vol. 42, N 9. P. 1687–1713. doi: 10.1016/s0735-1097(03)00941-0
- Kotkar K.D., Said S.M., Dearani J.A., Schaff H.V. Hypertrophic obstructive cardiomyopathy: the Mayo Clinic experience // Ann Cardiothorac Surg. 2017. Vol. 6, N 4. P. 329–336. doi: 10.21037/acs.2017.07.03
- Ommen S.R., Mital S., Burke M.A., et al. 2020 AHA/ACC Guideline for the Diagnosis and Treatment of Patients With Hypertrophic Cardiomyopathy: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines // Circultation. 2020. Vol. 142, N 25. P. e558–e631. doi: 10.1161/CIR.0000000000000937
- Brigden W. Uncommon myocardial diseases: the non-coronary cardiomyopathies // Lancet. 1957. Vol. 273, N 7008. P. 1243–1249. doi: 10.1016/s0140-6736(57)91537-4
- Choudhury L., Mahrholdt H., Wagner A., et al. Myocardial scarring in asymptomatic or mildly symptomatic patients with hypertrophic cardiomyopathy // J Am Coll Cardiol. 2002. Vol. 40, N 12. P. 2156–2164. doi: 10.1016/S0735-1097(02)02602-5
- Shiozaki A.A., Senra T., Arteaga E., et al. Myocardial fibrosis detected by cardiac CT predicts ventricular fibrillation/ventricular tachycardia events in patients with hypertrophic cardiomyopathy // J Cardiovasc Comput Tomogr. 2013. Vol. 7, N 3. P. 173–181. doi: 10.1016/j.jcct.2013.04.002
- Qin L., Chen C., Gu S., et al. A radiomic approach to predict myocardial fibrosis on coronary CT angiography in hypertrophic cardiomyopathy // International Journal of Cardiology. 2021. Vol. 337. P. 113–118. doi: 10.1016/j.ijcard.2021.04.060
- Berliner J.I., Kino A., Carr J.C., Bonow R.O., Choudhury L. Cardiac computed tomographic imaging to evaluate myocardial scarring/fibrosis in patients with hypertrophic cardiomyopathy: a comparison with cardiac magnetic resonance imaging // Int J Cardiovasc Imaging. 2013. Vol. 29, N 1. P. 191–197. doi: 10.1007/s10554-012-0048-y
- Бокерия Л.А. Гипертрофическая обструктивная кардиомиопатия // Анналы хирургии. 2013. Т. 5. С. 5–14.
- Baxi A.J., Restrepo C.S., Vargas D., et al. Hypertrophic cardiomyopathy from A to Z: genetics, pathophysiology, imaging, and management // Radiographics. 2016. Vol. 36. P. 335–354. doi: 10.1148/rg.2016150137
- Efthimiadis G.K., Pagourelias E.D., Hadjimiltiades S., et al. Feasibility and significance of preclinical diagnosis in hypertrophic cardiomyopathy // Cardiol Rev. 2015. Vol. 23, N 6. P. 297–302. doi: 10.1097/CRD.0000000000000076
- Васильев Ю.А., Семенов Д.С., Ахмад Е.С., и др. Особенности проведения магнитно-резонансной томографии у пациентов с имплантами и металлоконструкциями. Москва : Общество с ограниченной ответственностью «Издательские решения», 2022. EDN: WNQXXM
- Bandula S., White S.K., Flett A.S., et al. Measurement of myocardial extracellular volume fraction by using equilibrium contrast-enhanced CT: validation against histologic findings // Radiology. 2013. Vol. 269, N 2. P. 396–403. doi: 10.1148/radiology.13130130
- Бокерия Л.А., Дарий О.Ю., Макаренко В.Н., и др. Компьютерная и магнитно-резонансная томография гипертрофической кардиомиопатии. Учебно-методическое пособие. Москва : Национальный медицинский исследовательский центр сердечно-сосудистой хирургии имени А.Н. Бакулева, 2022. EDN: MOGFHL
- Patel P., Dhillon A., Popovic Z., et al. Left ventricular outflow tract obstruction in hypertrophic cardiomyopathy patients without severe septal hypertrophy: implications of mitral valve and papillary muscle abnormalities assessed using cardiac magnetic resonance and echocardiography // Circ Cardiovasc Imaging. 2015. Vol. 8, N 7. P. e003132. doi: 10.1161/CIRCIMAGING.115.003132
- Laaroussi L., Ben Halima A., Boukhris M. Left ventricular non-compaction associated with hypertrophic cardiomyopathy in the same patient // Kardiol Pol. 2017. Vol. 75, N 4. P. 397. doi: 10.5603/KP.2017.0064
- Wigle E.D., Auger P., Marquis Y. Muscular subaortic stenosis: the initial left ventricular inflow tract pressure as evidence of outflow tract obstruction // Can Med Assoc J. 1966. Vol. 95, N 16. P. 793–797.
- Ramsheyi S.A., Pargaonkar S., Lassau J.P., Acar C. Morphologic classification of the mitral papillary muscles // J Heart Valve Dis. 1996. Vol. 5, N 5. P. 472–476.
- Ковалевская Е.А., Крылова Н.С., Потешкина Н.Г., и др. Клинический профиль у больных гипертрофической кардиомиопатией с ишемией миокарда в отсутствие атеросклероза коронарных артерий // Лечебное дело. 2018. № 4. С. 36–42. EDN: VVQBKY
- Abadia A., Assen M., Martin S., et al. Myocardial extracellular volume fraction to differentiate healthy from cardiomyopathic myocardium using dual-source dual-energy CT // Journal of Cardiovascular Computed Tomography. 2020. Vol. 14, N 2. P. 162–167. doi: 10.1016/j.jcct.2019.09.008
- Vullaganti S., Levine J., Raiker N., et al. Fibrosis in Hypertrophic Cardiomyopathy Patients With and Without Sarcomere Gene Mutations // Heart Lung Circ. 2021. Vol. 30, N 10. P. 1496–1501. doi: 10.1016/j.hlc.2021.04.008
Дополнительные файлы









